A surgeon touches the screen to adjust a setting, leaving behind a smudge. A nurse quickly wipes it, but the resulting glare now obscures a critical part of the anatomical view.
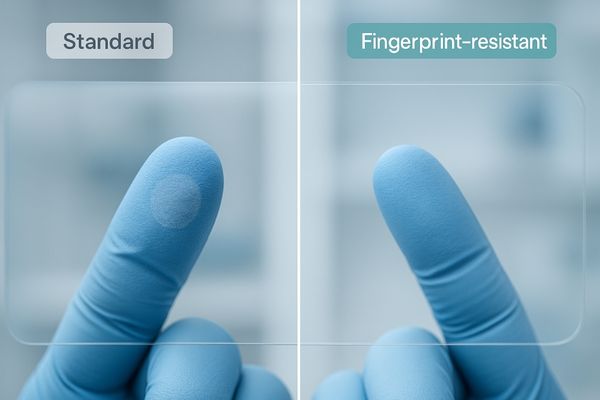
A fingerprint-resistant coating is a specialized top layer that repels oils and residues. When combined with anti-reflective glass and optical bonding, it maintains image clarity, reduces cleaning interruptions, and enhances durability.
Executive summary for decision-makers: better readability with fewer wipes, auditable acceptance metrics (contact angles, wipe cycles), and longer surface life that lowers TCO.
 Fingerprint-Resistant Coating in Action
Fingerprint-Resistant Coating in Action
When we evaluate surgical displays, we tend to focus on core specifications like 4K resolution, color accuracy, and brightness. These are undoubtedly vital, but a display’s long-term performance in the real world is often dictated by smaller, more practical features. One of the most overlooked yet impactful of these is the quality of the front surface coating. In the fast-paced, sterile environment of the operating room, displays are constantly being touched, wiped, and exposed to various substances. A simple fingerprint or a film of residue can degrade a multi-thousand-dollar display’s performance to the point of clinical irrelevance. Investing in a properly engineered, fingerprint-resistant surface1 is not a minor upgrade; it is a fundamental requirement for maintaining image integrity, operational efficiency, and patient safety.
What a fingerprint-resistant coating is
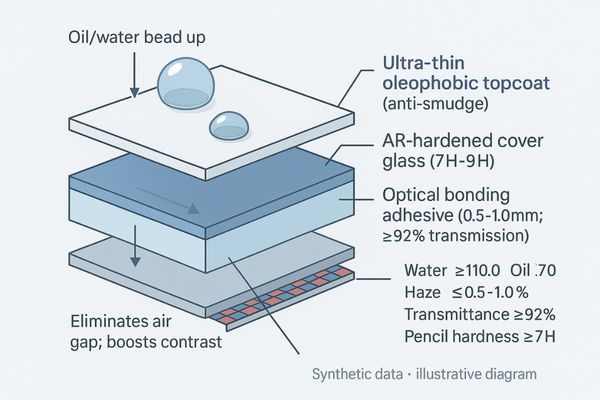
Start with definitions you can verify: an oleophobic topcoat, AR-hardened cover glass, and optical bonding measured by clear acceptance metrics.
A fingerprint-resistant coating is an oleophobic (oil-repelling) top layer paired with hardened, anti-reflective glass that maintains clarity and durability, measured by contact angle, hardness, and post-wipe light transmittance.
 The Science Behind a Fingerprint-Resistant Coating
The Science Behind a Fingerprint-Resistant Coating
A medical-grade fingerprint-resistant coating is a sophisticated surface treatment, not just a simple spray-on solution. At its core, it is an oleophobic coating, meaning it is engineered at a molecular level to have very low surface energy. This property makes it difficult for oils, such as those from fingerprints or glove residues, to adhere to the screen. Instead of smearing, oils tend to bead up and can be wiped away easily without leaving a hazy film.
Key Performance Metrics
The effectiveness of this coating is not subjective; it is measured by several key performance indicators2. The water and oil contact angles quantify how effectively the surface repels liquids—a higher angle means better repellency. Surface hardness, often measured on the Pencil Hardness Scale, indicates its resistance to micro-scratches from repeated wiping. Finally, metrics like haze and post-wipe transmittance verify that the coating does its job without degrading the optical quality of the display. For surgical use, this coating is typically applied as the final layer on top of a stack that includes Anti-Reflective (AR) treated, hardened cover glass and optical bonding for maximum performance.
- Procurement placeholders to confirm before publishing: Water ≥ 110°, Oil ≥ 70°; Haze ≤ 0.5–1.0%; Transmittance ≥ 92%; Pencil hardness ≥ 7H; IPA 70% ≥ 1,000 cycles; NaOCl 0.1% ≥ 500 cycles; H₂O₂ 1–3% ≥ 500 cycles; Quats (per vendor conc.) ≥ 1,000 cycles.
Why it matters in the OR
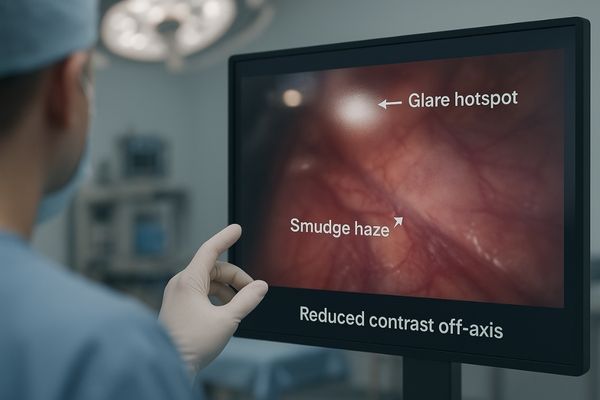
Keep screens readable with fewer wipes: smudge films raise glare and haze, reduce contrast, and hurt off-axis legibility.
Glove oils and residues create hazy films that increase glare, reduce image contrast, and impair off-axis readability. This forces repeated cleaning cycles, which interrupt the surgical flow and team focus.
 The Impact of Smudges on Off-Axis Readability in the OR
The Impact of Smudges on Off-Axis Readability in the OR
The operating room is a tactile environment. Even with no-touch techniques, displays are inevitably exposed to contaminants. Gloved hands, whether adjusting a boom arm, pointing out an anatomical feature, or interacting with a touch interface, can transfer oils, gels, and other residues onto the screen. On a standard glass surface, this buildup creates a greasy, highly reflective film.
The Degradation of Image Quality
This film has a direct and negative impact on image quality. It increases specular glare3 from the powerful overhead surgical lights, which can obscure critical details. It lowers the overall contrast of the image, making it harder to differentiate between subtle tissue variations. This problem is magnified when viewing the display from an off-axis angle, a common scenario for nurses, anesthesiologists, and other team members who are not standing directly in front of the screen. The constant need for wiping the screen is itself a problem. It interrupts the concentration of the circulating nurse and represents a break in workflow. Every moment spent cleaning the display is a moment not spent attending to the patient or the surgical team\’s needs.
Risks when protection is inadequate
Separate clinical risks, cleaning overhead, and surface wear—each can trigger system-level issues mid-procedure.
An unprotected screen leads to misreads of fine details, requires longer cleaning cycles with more consumables, and suffers from micro-scratches from aggressive wiping, creating a vicious cycle of faster contamination.
 The Vicious Cycle of Inadequate Screen Protection
The Vicious Cycle of Inadequate Screen Protection
Clinical and Team Risks
Glare and haze can obscure small vessels, nerves, or margins; surgeons either guess or pause for cleaning, increasing cognitive load and procedure time.
Cleaning Overhead and Consumables
Residues adhere strongly without an oleophobic surface4, demanding more wipes, stronger chemicals, and more interruptions that break surgical flow.
The Vicious Cycle of Degradation
Aggressive wiping introduces micro-scratches that scatter light and worsen haze; the roughened surface traps more oils, accelerating failure and shortening the display’s useful life.
A practical, verifiable solution
Engineer a three-layer system with clear acceptance criteria, chemistry compatibility, and traceable records.
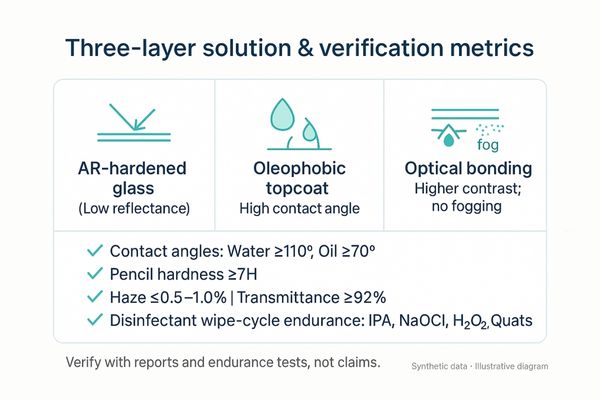
A robust solution is a three-layer stack of AR-hardened glass, an anti-smudge topcoat, and optical bonding, all verified with traceable reports on contact angles, hardness, and chemical wipe-cycle endurance.
 The Three-Layer Solution and its Verification Metrics
The Three-Layer Solution and its Verification Metrics
The Three-Layer Stack
The foundation of a practical solution is a three-part stack. It starts with an AR-hardened cover glass that provides a durable, scratch-resistant base with low reflectivity. This is then coated with the anti-smudge (oleophobic) topcoat5 to repel oils and residues. Finally, the entire assembly is attached to the LCD panel via optical bonding, which eliminates internal air gaps to improve contrast and prevent internal fogging.
Verification and Maintenance
This engineered solution must be verifiable. Procurement and acceptance should be based on objective data, not just marketing claims. This includes traceable reports specifying water/oil contact angles, pencil hardness rating, and, most importantly, wipe-cycle endurance against common hospital disinfectants (IPA, NaOCl, H₂O₂, quats). This ensures the coating not only works but will last. This technology should be paired with a clear cleaning SOP that uses approved chemicals and techniques to maximize the coating\’s lifespan and effectiveness.
RFP/Acceptance Checklist (submit with bids)
- Third-party or traceable reports for: water/oil contact angles, haze/transmittance, pencil hardness.
- Approved/forbidden disinfectant list with concentrations and tested wipe cycles.
- Post-endurance retention (contact angle/transmittance) curves or tabulated deltas.
- Cleaning SOP including wipe order, dwell time, drying time, pressure/velocity limits, and inspection cadence.
- Test artifacts: before/after photos, sample IDs, dates, signatures.
Disinfectant & Cleaning Acceptance Log (template)
| — |
|---|
Recommended Surgical Displays with Enhanced Surface Durability
| — | ||||||
|---|---|---|---|---|---|---|
| MS321PB | Main Surgical Display (4K) | Designed for tower/boom arms, with options for optical bonding and an easy-to-clean front surface (check specs). | ||||
| MS220SA | Compact & Mobile Display (FHD) | Ideal for mobile carts and information display, where its smaller surface is quick to wipe and maintain. | ||||
| MS550P | Wall-Mounted Team Display (4K) | A flat front surface simplifies rapid decontamination and disinfection, crucial for shared viewing environments. | ||||
| MS270P | Auxiliary/Teaching (FHD) | 27" class for secondary viewing and training; verify anti-smudge option and bonding per current datasheet. |
For specs or disinfectant whitelist, contact info@reshinmonitors.com.
Measurable business value
Translate surface engineering into KPIs: fewer interruptions, longer surface life, and predictable room turnover.
Fewer cleaning interruptions, sustained image readability, and slower surface aging reduce maintenance and consumables costs. This leads to smoother teamwork and more predictable room turnover, lowering the overall TCO.
 The Measurable Business Value of Durable Coatings
The Measurable Business Value of Durable Coatings
Typical outcomes to validate during pilots: cleaning interruptions ↓30–50%; wipe consumables ↓20–40%; surface-related service tickets ↓10–20% (fill with your trial data before publishing).
FAQ
Does a fingerprint-resistant coating reduce the display\’s clarity?
No. When properly integrated with an Anti-Reflective (AR) layer and optical bonding, a high-quality oleophobic coating should have no negative impact on resolution or clarity. Key specifications to check are the coating\’s haze and light transmittance values, which should be minimal.
Action: request haze/transmittance reports and full-resolution image/MTF captures pre/post endurance.
How long does the coating last?
The lifespan depends heavily on the cleaning agents used and the frequency and force of the wiping. A medical-grade coating should be specified to withstand thousands of wipe cycles with approved hospital disinfectants. Acceptance criteria should include post-endurance metrics that show how much performance (e.g., contact angle) is retained.
Action: require wipe-cycle counts by agent, plus retention curves and pass/fail thresholds in the contract.
How is a medical-grade coating different from what\’s on my phone?
The primary difference is the focus on chemical resistance and auditable testing. While a consumer coating is designed to resist fingerprints, a medical-grade coating must also withstand repeated disinfection with harsh chemicals like bleach and alcohol without degrading, and this performance must be backed by verifiable test data.
Action: compare the vendor’s approved disinfectant whitelist and cycle counts against your hospital’s policy.
Conclusion
Treat anti-smudge topcoats, AR glass, and optical bonding as a baseline system, using verifiable metrics and SOPs to make a "clean and readable" display a measurable and repeatable standard.
- Explore how a fingerprint-resistant surface can enhance display performance and ensure patient safety in surgical environments. ↩
- Learn about the essential metrics that determine the effectiveness of coatings in medical settings, ensuring optimal performance. ↩
- Exploring the effects of specular glare can lead to better lighting solutions and improved visibility during surgeries. ↩
- Exploring oleophobic surfaces can enhance surgical performance by reducing cleaning time and improving visibility. ↩
- Discover how an anti-smudge oleophobic topcoat enhances durability and cleanliness in various applications. ↩


