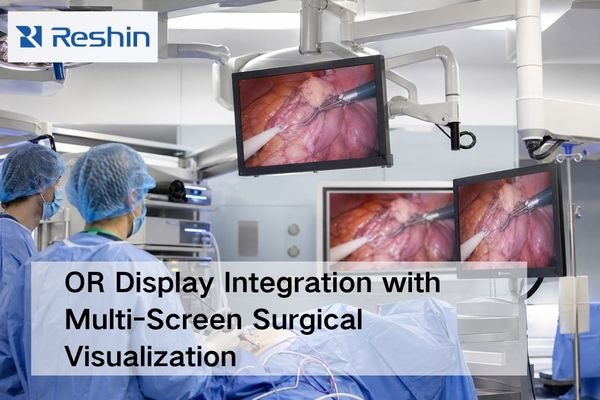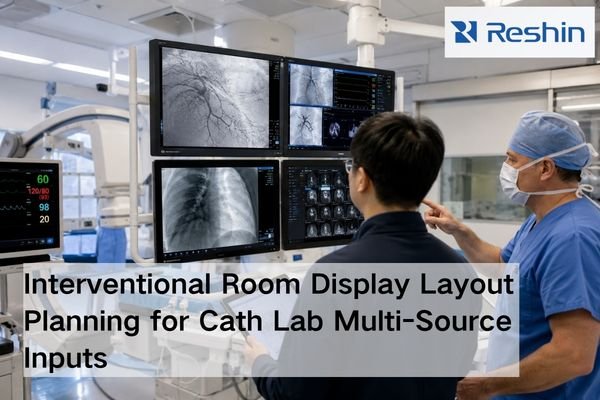
Interventional Room Display Layout Planning: Main View, Review View and Multi-Source Inputs
Interventional room display layout planning should follow five steps: define display roles, list all source signals, map routing paths, validate viewing position and mounting, and freeze the approved layout package before installation. Main view, review view, and multi-source inputs should be confirmed before model selection expands.