A surgeon adjusts the endoscope, trying to get a better view, but the image on the display remains washed out or plunged in shadow. The instinctive reaction is to blame the camera.
When surgeons report that an image is "too bright" or "too dark," they are often describing a loss of detail due to highlight clipping, black crush, or incorrect mid-tones caused by misconfigurations in the video chain.
In the operating room, image quality1 is not a luxury; it is a prerequisite for safe and effective surgery. While a camera’s auto-exposure can contribute, “too bright/dark” complaints often indicate a deeper pipeline issue. The problem frequently lies in the chain of devices that process and transport the video signal to the display. Mismatched color space, video range, and gamma can crush, clip, or distort the image in ways that endoscope adjustments cannot fix. The goal is a verifiable, end-to-end video pipeline that delivers a consistent, accurate image every time.
What do “too bright/dark” complaints really mean?
A short complaint masks a tonal-reproduction failure: lost highlights, crushed shadows, or wrong mid-tones—not just “overall brightness.”
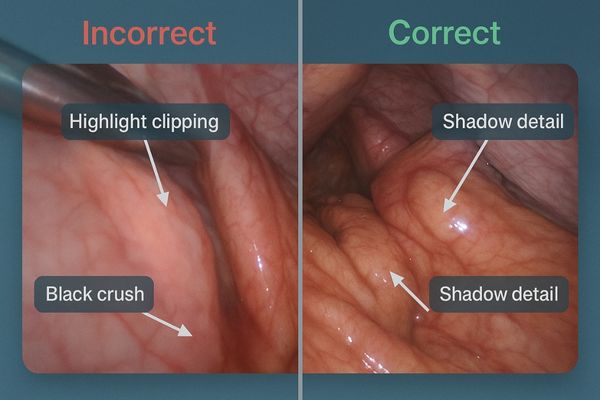
"Too bright/dark" signifies a loss of diagnostic detail. "Too bright" means highlight clipping, while "too dark" means black crush. Both are often symptoms of mismatched signal-processing settings.
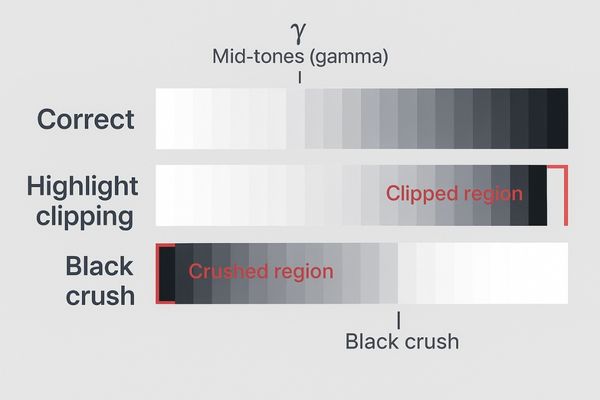
When a surgeon says the image is "too bright," they rarely mean the entire picture is overexposed. More accurately, they are observing that the brightest parts have lost detail and turned into a flat white—highlight clipping. This is dangerous in endoscopy, where specular reflections are common; a small lesion within that reflective area can vanish. Conversely, "too dark" points to black crush2, where shadow areas collapse into featureless black, erasing the low-contrast textures needed to differentiate tissue planes. Incorrect gamma (mid-tones) can also make tissue look flat or “plastic,” altering depth and texture. These are data-processing errors, not exposure alone.
Root causes beyond the endoscope: chain misconfigurations
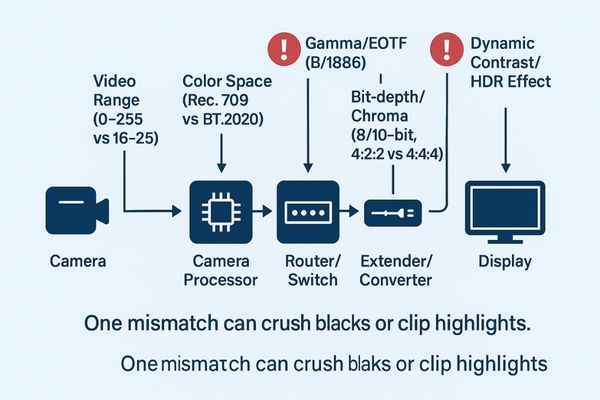
The same signal must be interpreted identically from source to display; any mismatch reshapes tones and colors.
Common culprits are mismatched full vs. limited video ranges, incorrect color space or gamma settings, bit-depth inconsistencies, and "image enhancement" features like dynamic contrast that corrupt the original signal.
Mismatches in signal definition
- Video range mismatch: limited (16–235) vs full (0–255). Limited → full causes washed blacks; full → limited causes crushed blacks and clipped whites.
- Color space and gamma mismatch3: most SDR scopes are Rec.709 with a defined EOTF (e.g., BT.1886). If the display expects BT.2020 or a different gamma, colors skew and tones shift.
Processing and enhancement errors
Bit-depth or chroma inconsistencies (8-bit vs 10-bit; 4:2:2 vs 4:4:4) add artifacts. Consumer “enhancements” (Dynamic Contrast, Local Dimming, HDR Effect) constantly alter brightness/contrast and corrupt the source signal.
One weak link—camera, processor, transport, display, or environment—breaks the whole chain.
Clinical impact: flattened cues and biased decisions
If tones are wrong, small but critical visual cues disappear; team timing and confidence degrade.
Highlight clipping can hide lesions, black crush obscures tissue textures, and incorrect gamma distorts appearance. This leads to misinterpretation, increases cognitive load, and prolongs procedure times.

Highlight clipping around specular reflections4 can obscure small polyps, vessels, or tumor margins, risking missed diagnosis or incomplete resection. Black crush erases low-contrast textures in shadowed cavities, masking safe dissection planes.
Incorrect gamma alters the apparent color and texture of tissue, making interpretation harder and increasing cognitive load as surgeons compensate mentally. Inconsistent presets across rooms desynchronize cues and disrupt workflow, extending procedure time and elevating error risk.
The fix: lock color space/range/gamma and disable gimmicks
Replace ad-hoc tweaks with a documented, testable signal policy—standardize, lock, and verify.
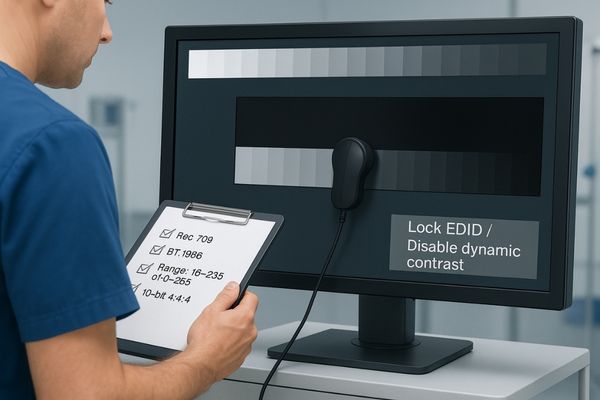
Enforce a consistent and verifiable signal chain: align on a standard color space, EOTF, and video range; lock settings end-to-end; disable all dynamic "enhancement" DSP; and calibrate using standard test patterns.
Establishing a standardized signal path
Standardize on Rec.709 for SDR endoscopy, a consistent EOTF (e.g., BT.1886), white point D65, and one video range (limited 16–235 or full 0–255) applied identically across all devices. Use EDID management to prevent silent re-negotiation and configure an end-to-end 10-bit, 4:4:4 pipeline where possible.
Disabling destructive processing and verifying performance
Disable Dynamic Contrast5, HDR simulation, aggressive edge enhancement, and non-native scaling where not required. Verify with PLUGE (black level) and grayscale step charts (white clip, mid-tone smoothness). Save these as a named preset (e.g., OR-Rec709-LIM-BT1886-D65) and record date/device/operator.
Required (do)
- Use Rec.709 + BT.1886 + D65 across the chain
- Lock one video range and keep it consistent end-to-end
- Ensure 10-bit 4:4:4; lock EDID/bit-depth
- Calibrate with PLUGE/grayscale; save presets and logs
- Control ambient light and reflections in the room
Do not (avoid)
- Mixing full and limited ranges
- Treating SDR as HDR or enabling “HDR effects”
- Forcing BT.2020 on Rec.709 sources
- Over-sharpening, aggressive dynamic contrast, non-native scaling
Quick self-check matrix (fill during acceptance)
| Item | Target/Setting | Result | Notes | Signed |
|---|---|---|---|---|
| Color space | Rec.709 | |||
| Gamma/EOTF | BT.1886 | |||
| White point | D65 | |||
| Range | 16–235 or 0–255 (一致) | |||
| Chroma/Bit-depth | 4:4:4 / 10-bit | |||
| PLUGE | No crush | |||
| Grayscale steps | No clip; smooth | |||
| Ambient light | Controlled |
Recommended Surgical Displays for Signal Integrity
| Model | Category | Key Features for Signal Management |
|---|---|---|
| MS322PB | Tower/Boom Main Display (4K) | Multiple inputs and layout templates; lockable Rec.709/EOTF, range, and presets with logging. |
| MS550P | Wall-Mounted Team Display (4K) | Consistent brightness and tone for team viewing; stable reference for side-by-side comparisons. |
| MS220SA | Compact/Auxiliary Display (FHD) | Ideal for auxiliary/teaching; quick PLUGE/grayscale self-checks to enforce unified presets. |
Business value: fewer re-works, fewer disputes, higher throughput
Consistent presets transform complaints into data, reducing troubleshooting and accelerating turnover.
Standardizing image reproduction turns subjective complaints into objective data, cutting down on troubleshooting, rework, and interdepartmental disputes, which in turn increases OR efficiency and lowers TCO.
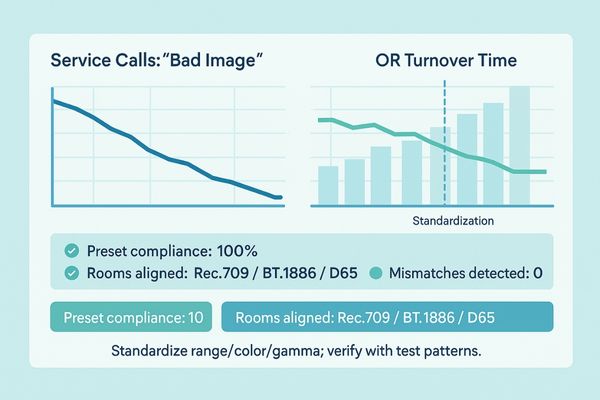
A verifiable pipeline reduces “bad image” tickets and frees biomed/IT for higher-value work. Objective standards minimize debates among clinicians, technicians, and vendors, shorten onboarding for new staff, and improve cross-room consistency. Hidden costs from inconsistent images decline, lowering and stabilizing total cost of ownership.
FAQ
Should I turn on "Dynamic Contrast" or "HDR Effect" for a better image?
For SDR endoscopy sources, disable these features. They alter the image unpredictably and can hide or exaggerate details. Use a standard Rec.709 profile with a fixed EOTF.
Is a full video range (0–255) always better than a limited range (16–235)?
Not necessarily. Consistency across the chain matters most. Full/limited mismatches are a common cause of crushed blacks or washed-out images.
How can I do a quick self-check of my display’s settings?
Use PLUGE to set black correctly without crush, and a grayscale step chart to confirm no highlight clipping and smooth mid-tones. Log the settings that work.
Should I set the color space to BT.2020 to get more colors?
Only if your source truly outputs BT.2020. Most SDR endoscopes are Rec.709. Forcing wider color spaces on Rec.709 sources causes color shifts and over-saturation.
Conclusion
By locking color space, video range, and gamma, standardizing calibration procedures, and controlling the room environment, subjective complaints become objective, repeatable imaging performance. 🎨
- Standardize Rec.709 + BT.1886 + D65
- Lock video range and EDID; ensure 10-bit 4:4:4
- Verify with PLUGE/grayscale and log presets
👉 For expert support and Reshin’s color-calibrated medical display solutions, contact info@reshinmonitors.com.
-
Understanding the significance of image quality can enhance surgical outcomes and patient safety ↩
-
Exploring black crush helps in recognizing its impact on tissue visibility, essential for accurate diagnosis and treatment. ↩
-
Exploring color space and gamma mismatch can help you optimize your video settings for accurate color representation. ↩
-
Understanding specular reflections can help improve diagnostic accuracy and surgical outcomes. ↩
-
Exploring the impact of Dynamic Contrast can help you avoid common pitfalls in video processing. ↩


