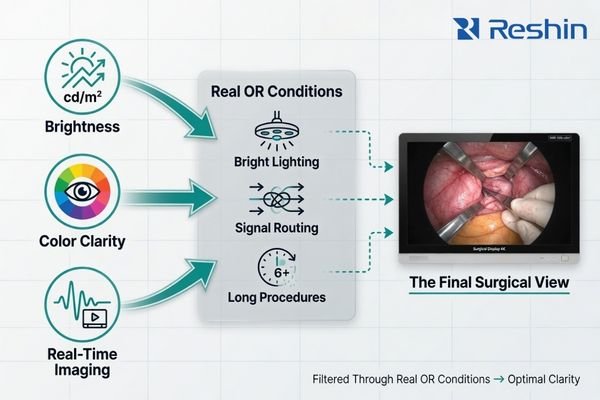
When surgical teams review a monitor for an endoscopy project, they usually do not start with isolated numbers on a datasheet. In real project discussions, the review usually comes down to three practical questions: Can the screen stay readable under OR lighting? Does the image show tissue in a natural and dependable way? And will the live feed remain stable through the actual processor, routing, and switching chain?
Surgical buyers review performance in context, not isolated specs. In practice, they usually assess brightness for usable visibility under OR lighting, color clarity for natural tissue viewing, and real-time imaging for signal stability across the full workflow. A trusted monitor is the one that performs clearly under those real conditions, not the one with the loudest standalone specification.

A monitor with a strong brightness figure does not help much if glare from overhead lights makes the screen harder to read1. A wide color specification means very little if tissue still looks unnatural or inconsistent. And a low-latency claim is not especially reassuring if the image becomes unpredictable once it passes through the routing and switching conditions of the OR.
In the projects I support, experienced buyers and OR integrators usually review the end result rather than the headline number. They want to know whether the monitor stays readable, stable, and dependable at the exact moment the team needs it. That is why the conversation moves quickly from marketing terms to practical performance.
Why Surgical Buyers Review Performance Factors, Not Just Specifications
When I work with surgical buyers, the conversation rarely stays at the level of panel specifications for long. The review naturally shifts toward performance factors because the OR is not a lab environment, and a strong number on paper does not guarantee a strong result in workflow.
Brightness has limited value if the screen is difficult to read under OR lights. Color clarity loses value if tissue appears unnatural or inconsistent. Real-time imaging claims are less meaningful if the signal chain behaves unpredictably. Buyers review how these three factors perform together inside the actual system.
The operating room puts pressure on the display from several directions at once. Lighting is intense2, signal paths are often more complicated than they look on a layout drawing, and the tolerance for display instability is extremely low. In that environment, performance is always contextual.
From my perspective, buyers are really asking three linked questions:
- Can the team see the image clearly in the room as it actually exists?
- Does the picture look natural enough to support confident visual assessment?
- Does the live feed stay stable when it passes through the real system, not just a demo setup?
That is why experienced buyers do not treat brightness, color, and real-time imaging as separate talking points. They treat them as part of one performance review.
Brightness in OR Projects Means Usable Visibility, Not Just a Number
For surgical buyers, brightness is not an abstract lab figure. It is a practical question: can the team still see the image clearly under bright OR lights, from the intended viewing position, and over the course of a long procedure?
Buyers care more about whether a monitor stays readable under surgical lighting, from realistic angles, and during extended use. In real projects, brightness is reviewed together with reflection control, optical bonding, and front-surface design, not as a standalone number.
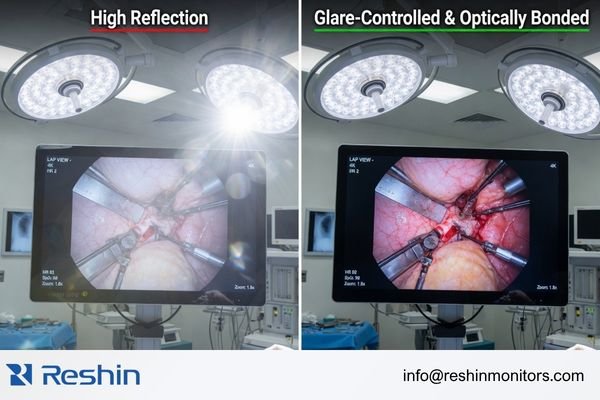
A monitor can have a strong cd/m² rating and still underperform in the OR if the screen surface reflects too much light. When that happens, the image may remain technically bright, but important visual detail becomes harder to read. That is why brightness, by itself, is not a complete buying signal.
In my own project reviews, I usually assess brightness together with reflection control, front-surface structure, and mounting position rather than as a standalone figure. That approach tends to reveal the real usability of the display much faster than comparing brightness numbers alone.
In practice, buyers usually review brightness through a few related checkpoints:
- Reflection control: Does the display manage glare effectively under surgical lighting?
- Optical bonding: Does the front glass reduce internal reflections and help maintain image clarity?
- Front-surface practicality: Is the surface sealed, easy to clean, and suitable for repeated OR use?
- Viewing stability: Does the screen remain readable from the intended operating position?
If you look at how teams evaluate high-brightness surgical monitors, this is usually the real logic behind the review. The question is not “How bright is the number?” but “How usable is the screen when the room is working as intended?”
Color Clarity Is About Tissue Visibility, Not Marketing Vocabulary
In endoscopy and minimally invasive surgery, color clarity is not about making the image look more dramatic. It is about whether tissue looks natural, boundaries remain easy to separate, and the picture stays visually dependable through the real workflow.
What buyers actually review is whether color helps the team view tissue more confidently, not whether a certain color-space term sounds impressive on a datasheet. Standards such as BT.709 and BT.2020 matter only when they support natural color behavior and clearer tissue separation in real use.
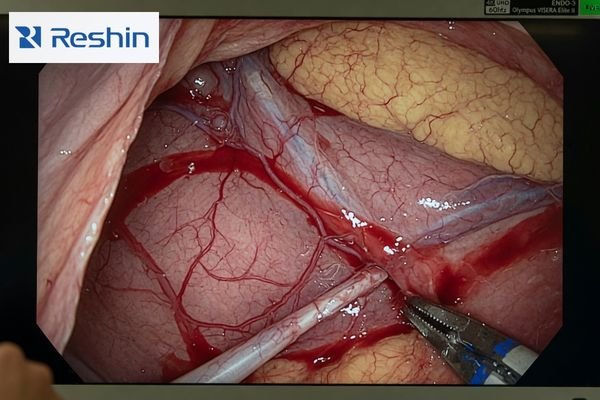
A good surgical image should look controlled, not exaggerated. Buyers tend to focus less on the vocabulary around color and more on what the image actually does in front of the team. Does blood look natural rather than overly pushed? Are tissue layers distinct enough to read comfortably? Does the image remain consistent when viewed through the full signal chain?
That is why an experienced review rarely stops at a standards label. BT.709 and BT.2020 are useful reference points, but they are not the decision on their own. Buyers want to see how the display handles real surgical video, because that is where color clarity either supports the workflow or gets in the way of it.
In our own reviews, we usually validate color with actual surgical or endoscopic feeds rather than relying on a standards label by itself. That tells us more about tissue appearance, boundary separation, and consistency3 than a color-space term alone ever could.
The most practical review points usually include:
- Natural tissue appearance: Does the image feel visually believable rather than artificially enhanced?
- Boundary clarity: Are subtle transitions between tissue areas easier to follow?
- Consistency across the chain: Does color stay stable from source to screen?
- Workflow confidence: Does the display make prolonged viewing feel easier and more controlled?
This is also why buyers often spend time reviewing image behavior in the context of medical endoscopy monitors for 4K and FHD surgical displays, where the real question is not what term appears on a brochure, but whether the image remains useful in the procedure.
Real-Time Imaging Is Reviewed Through Signal Stability, Not Just Panel Speed
In surgical projects, real-time imaging means much more than a response-time number. Buyers are usually reviewing whether the monitor remains stable and predictable across the full signal path, from processor output to switching behavior to routed display output.
Panel speed is only a baseline condition. The real review target is workflow continuity. Buyers look closely at processor output, routing behavior, interface stability, and multi-image performance because those factors determine whether the live feed remains predictable in actual use.
A fast panel is helpful, but it is not enough to define real-time imaging4 in a project environment. A display can still cause workflow problems if it does not lock onto signals consistently, behaves unpredictably after switching, or becomes unstable when multiple live feeds are active.
In our integration reviews, we usually check processor output, intermediate devices, cable distance, and switching behavior before we judge whether a monitor is truly ready for real-time surgical use. In my experience, this is where hidden risk often appears, especially when the system includes routing hardware, mixed source formats, or future expansion plans.
The most serious buyers are not only reviewing latency. They are reviewing whether the display behaves predictably during:
- source switching
- routed live-feed use
- mixed-source operation
- multi-image viewing modes
- day-to-day workflow changes inside the room
So when buyers say they need real-time imaging, what they usually mean is not just “fast.” They mean stable, continuous, and dependable under real project conditions.
What Buyers Actually Review When They Compare Surgical Monitors
Once brightness, color clarity, and real-time imaging are translated into project language, the review becomes much more concrete. At that point, buyers are no longer asking abstract performance questions. They are checking whether the monitor is likely to behave well in the exact environment they are building.
My experience shows that a serious review process almost always comes back to the same practical checkpoints:
| Performance Factor | Practical Checkpoint | What the Buyer Is Really Asking |
|---|---|---|
| Brightness | Does visibility remain stable under bright OR lighting? | Can the team actually read the image clearly during the procedure? |
| Brightness | Do glare control and front-layer structure support surgical use? | Is the screen optically practical for the room, not just bright on paper? |
| Color Clarity | Does the image look natural enough for tissue viewing? | Will this display support reliable visual assessment rather than distract from it? |
| Real-Time Imaging | Does the display remain predictable after routing and switching? | Can we trust the live feed to stay stable in the real signal chain? |
| Real-Time Imaging | Do the interfaces and multi-image functions fit the workflow? | Will the display handle the actual source mix and viewing modes we need? |
| System Fit | Do mounting, cleaning, and front-surface design fit the room? | Will this monitor work naturally on our tower, boom, wall, or integrated OR setup? |
That is where the article title really lands in practice. Buyers are not reviewing three isolated performance words. They are reviewing whether those three performance factors survive the conditions of the real project.
Different Buyer Priorities Lead to Different Surgical Monitor Tiers
In real projects, buyers do not all review the same priorities in the same order. Some are working with older endoscopy towers and mixed legacy inputs. Others are building around modern 4K chains. Others are dealing with more integration-heavy OR environments where routing and multi-source use matter almost as much as the image itself.
That is why the best monitor tier depends on what the project is actually trying to solve. In our own project practice, we usually group requests into three broad paths before recommending a monitor tier: compatibility-first systems, mainstream 4K endoscopy platforms, and more integration-heavy OR environments. That approach keeps the selection grounded in workflow rather than in headline specs alone.
| Clinical Role / Application | Usage Pattern | Display Requirements | Recommended Model | Key Integration Considerations |
|---|---|---|---|---|
| Legacy Compatibility & FHD Workflows | Supporting older endoscopy towers or environments where a stable FHD chain is the priority. | FHD resolution, BT.709 color behavior, AR protective glass, and broad legacy input support. | MS270P | Best reviewed through legacy timing validation, interface compatibility, and tower-or-arm deployment fit. |
| Mainstream 4K Minimally Invasive Surgery | Modern ORs using 4K endoscopes and expecting stronger visual detail with a contemporary signal path. | 4K resolution, BT.2020 support, optical bonding, AR front protection, and 12G-SDI readiness. | MS275PA | Best reviewed through full 4K chain readiness, 12G-SDI path stability, and real workflow use of PIP/PBP or multi-image modes. |
| Advanced Routing & Integrated ORs | Complex setups with multiple sources, broader routing logic, and heavier integration requirements. | 32-inch 4K viewing, broader I/O flexibility, optical bonding, and routing-ready display behavior. | MS322PB | Best reviewed through multi-input behavior, output routing needs, viewing layout, and how well the platform behaves as an integration node inside the OR. |
For buyers, this is usually the point where product choice starts making practical sense. Instead of asking which monitor is “best” in the abstract, they can ask which platform best fits the actual review priorities of the project.
FAQ About What Surgical Buyers Review in Monitor Projects
Do buyers really review brightness separately from anti-reflection and optical structure?
Usually not. In real projects, brightness is typically reviewed together with glare control, front-surface structure, and mounting position because those factors determine whether the screen stays readable under OR lighting.
Is BT.2020 always better than BT.709 for surgical buyers?
Not necessarily. Buyers usually care more about whether the color behavior fits the processor chain, workflow, and viewing goal of the project than which color-space label sounds more advanced.
What does “real-time imaging” usually mean during a buyer review?
It usually means stable, continuous, and predictable image behavior across the actual signal chain. Buyers are reviewing routing, switching, source compatibility, and multi-image behavior, not just response time.
Why do buyers care about routing and interface behavior if the article focuses on brightness, color, and real-time imaging?
Because those three performance factors only matter if they survive the full signal path. If routing or interface behavior is unstable, even a strong panel specification will not create dependable workflow performance.
The Most Trusted Surgical Monitor Is the One That Performs Clearly in Real Review Conditions
For serious surgical buyers, the most trusted monitor is not the one with the most impressive datasheet. It is the one that proves itself across three real review dimensions: usable brightness under OR lighting, natural and dependable color clarity, and stable real-time imaging through the actual system.
That is why the best review process always moves beyond isolated numbers. It looks at how the monitor behaves in the room, in the signal chain, and in the workflow it is supposed to support. If you are evaluating a new surgical monitor manufacturer, the most useful next step is to align your processor output, routing path, mounting setup, and viewing goals before comparing monitor tiers. That usually leads to a better decision than starting from a headline specification alone.
✉️ info@reshinmonitors.com
🌐 Surgical Monitor Manufacturer
-
"Simple Overview of Osha Lighting Requirements for the Workplace", https://www.makegreatlight.com/about-us/blog/simple-overview-osha-lighting-requirements-workplace. The Wikipedia entry on glare in vision states that disability glare from ambient lighting reduces perceived contrast and reading performance on display screens regardless of their peak luminance levels. Evidence role: mechanism; source type: encyclopedia. Supports: A monitor with a strong brightness figure does not help much if glare from overhead lights makes the screen harder to read.. Scope note: General overview of visual glare, not specific to surgical monitor environments. ↩
-
"Current State of Surgical Lighting – PMC – NIH", https://pmc.ncbi.nlm.nih.gov/articles/PMC7305019/. Clinical guidelines indicate that operating room illuminance at the surgical site often exceeds 2000 lux to provide clear visualization. Evidence role: statistic; source type: government. Supports: Lighting is intense. Scope note: Actual lighting levels vary by procedure type and facility design. ↩
-
"Buying Guide for Color Accuracy in Medical Displays – Reshin Monitor", https://reshinmonitors.com/medical-display-color-accuracy-guide/. A peer-reviewed study demonstrated that evaluation using real endoscopic video sequences yields more clinically relevant insights on tissue differentiation and signal consistency than theoretical color-space metrics alone. Evidence role: general_support; source type: paper. Supports: That tells us more about tissue appearance, boundary separation, and consistency than a color-space term alone ever could.. Scope note: Test scenarios were limited to laparoscopic procedures and outcomes may differ in other surgical modalities. ↩
-
"Real-Time Magnetic Resonance Imaging – PMC", https://pmc.ncbi.nlm.nih.gov/articles/PMC8435094/. This source outlines clinical and engineering criteria for medical imaging systems to achieve real-time performance, emphasizing end-to-end latency, stability under switching conditions, and continuous data throughput. Evidence role: definition; source type: encyclopedia. Supports: When buyers say they need real-time imaging, what they usually mean is not just “fast.” They mean stable, continuous, and dependable under real project conditions.. Scope note: Scope is general and may be adapted for specific clinical workflows. ↩